Filter
274
Filtered Results: 274
Text search:
maladies
cardiovasculaires
Featured
Recommendations
28
New Publications
57
Language
Document type
No document type
114
Guidelines
57
Studies & Reports
53
Strategic & Response Plan
13
Fact sheets
13
Manuals
12
Infographics
5
Situation Updates
3
Training Material
2
Brochures
1
Resource Platforms
1
Countries / Regions
Senegal
20
Benin
15
Global
15
Congo, Democratic Republic of
14
Burkina Faso
12
Haiti
8
Latin America and the Carribbean
8
Togo
6
Cameroon
6
Niger
4
Africa
4
Luxembourg
4
Central African Republic
4
West and Central Africa
3
East and Southern Africa
3
Mali
3
Madagascar
3
Burundi
2
Middle East and North Africa
2
Western and Central Europe
2
France
2
Bolivia
2
Brazil
2
Colombia
1
Rwanda
1
Canada
1
Congo-Brazzaville
1
Guinea
1
Germany
1
Belgium
1
Côte d’Ivoire / Ivory Coast
1
South Africa
1
Eastern Europe
1
Djibouti
1
Chad
1
Ecuador
1
India
1
Bahamas
1
Authors & Publishers
Publication Years
Category
Countries
100
Clinical Guidelines
68
Public Health
27
Women & Child Health
6
Key Resources
5
Capacity Building
2
Pharmacy & Technologies
2
Toolboxes
NCDs
35
COVID-19
34
Mental Health
21
Caregiver
13
Planetary Health
9
NTDs
7
Disability
5
HIV
4
TB
4
Rapid Response
3
Refugee
2
Pharmacy
2
Global Health Education
2
Natural Hazards
1
Ebola & Marburg
1
Conflict
1
Desde el 2016, la Organización Panamericana de la Salud (OPS) ha promovido la implementación de la Iniciativa HEARTS en las Américas, una adaptación regional de la estrategia Global HEARTS de la Organización Mundial de la Salud (OMS). Durante este tiempo, 33 países de la Región de las Améric...

Socioeconomic status is associated with differences in risk factors for cardiovascular disease incidence and outcomes, including mortality. However, it is unclear whether the associations between cardiovascular disease and common measures of socioeconomic status—wealth and education—differ among...

Patients with diabetes are at increased risk of developing cardiovascular disease (CVD) with its manifestations of coronary artery disease (CAD), heart failure (HF), atrial fibrillation (AF), and stroke, as well as aortic and peripheral artery diseases. In addition, diabetes is a major risk factor f...
Approximately 80% of the 463 million adults worldwide with diabetes live in low-income and middle-income countries (LMICs). A major obstacle to designing evidence-based policies to improve diabetes outcomes in LMICs is the scarce availability of nationally representative data on the current patterns...

Non-Communicable Diseases (NCDs) are a worldwide epidemic. Particularly, the most common diseases - Cardiovascular diseases, Chronic Obstructive Pulmonary Diseases (COPD), Chronic Kidney Diseases, Cancer, Diabetes, injuries and disabilities, EMT, oral, eye g...

Chronic respiratory diseases, such as asthma and
chronic obstructive pulmonary disease, kill more than
four million people every year and affect hundreds
of millions more. These diseases erode the health
and well-being of the patients and have a negative
impact on families and societies. Women ...
El documento, "Progreso en la prevención y el control de las enfermedades no transmisibles" (ENT), informa sobre los esfuerzos globales para reducir el impacto de las ENT, como las enfermedades cardíacas, el cáncer, la diabetes y las enfermedades respiratorias crónicas, siguiendo los compromisos...

Excessive consumption of salt (more than 5 g per day) raises blood pressure, a major risk factor for cardiovascular diseases such as heart disease and stroke, and is the leading cause of death in the WHO European Region. Many countries in the Region have initiated national salt reduction strategies,...
Cardiovascular diseases, principally ischemic heart disease (IHD), are the most important cause of death and disability in the majority of low- and lower-middle-income countries (LLMICs). In these countries, IHD mortality rates are significantly greater in individuals of a low socioeconomic status (...
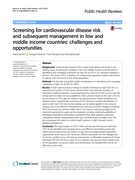
Background: Cardiovascular disease (CVD), mainly heart attack and stroke, is the
leading cause of premature mortality in low and middle income countries (LMICs).
Identifying and managing individuals at high risk of CVD is an important strategy to prevent and control CVD, in addition to multisector...

The incidence and mortality of cardiovascular diseases (CVDs) in low and middle income countries (LMICs) have been increasing, while access to CVDs medicines is suboptimal. We assessed selection of essential medicines for the prevention and treatment of CVDs on national essential medicines lists (NE...

In this document, the Inter-American Committee of Cardiovascular Prevention and Rehabilitation, together with the South
American Society of Cardiology, aimed to formulate strategies, measures, and actions for cardiovascular disease prevention
and rehabilitation (CVDPR). In the context of the imple...
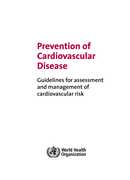
Cardiovascular disease is a major cause of disability and premature death throughout the world, and contributes substantially to the escalating costs of health care. The underlying pathology is atherosclerosis, which develops over many years and is usually advanced by the time symptoms occur, genera...
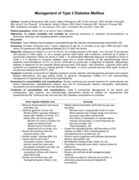
The document "Management of Type 2 Diabetes Mellitus" provides comprehensive guidelines for the diagnosis, prevention, and treatment of type 2 diabetes in adults. It emphasizes the importance of individualized glycemic targets, lifestyle interventions like diet and exercise, and the use of medicatio...
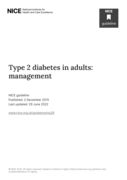
This guideline covers care and management for adults (aged 18 and over) with type 2 diabetes. It focuses on patient education, dietary advice, managing cardiovascular risk, managing blood glucose levels, and identifying and managing long-term complications.

The document provides the NICE Quality Standard for managing Type 2 diabetes in adults (QS209). It outlines evidence-based recommendations for preventing Type 2 diabetes, structured education, continuous glucose monitoring (CGM), medication such as SGLT2 inhibitors, and regular care processes to mon...
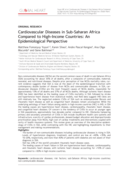
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...
Volume 1 covers emergency triage assessment and treatment, and acute care for a severely ill or acutely injured patient for approximately the first 24 hours of care. It describes the clinical procedures commonly used in emergency and acute care, and gives a summary of the medicines used and the step...

The South African (SA) guidelines for cardiac patients for non-cardiac surgery were developed to address the need for cardiac risk assessment and risk stratification for elective non-cardiac surgical patients in SA, and more broadly in Africa.
The guidelines were developed by updating the Canadian ...

Lancet 2012; 380: 611–19
Series: Hypertension 3