Filter
12
Filtered Results: 12
Text search:
D.
P.
Chin,
C.
L.
Hanson
Featured
New Publications
3
Language
Document type
No document type
6
Studies & Reports
5
Manuals
1
Countries / Regions
Africa
2
Ghana
1
Global
1
Western and Central Europe
1
Eastern Europe
1
Russia
1
Authors & Publishers
Publication Years
Category
Public Health
3
Countries
2
Clinical Guidelines
2
Women & Child Health
1
Key Resources
1
Toolboxes
Social Ethics
2
NCDs
2
TB
1
Caregiver
1
Planetary Health
1
NTDs
1

Supplement article
The Journal of Infectious Diseases® 2017;216(S7):S675–8
DOI: 10.1093/infdis/jix368
Finding the Missing Tuberculosis Patients • JID 2017:216 (Suppl 7) • S675
Downloaded from https://academic.oup.com/jid/article-abstract/216/suppl_7/S675/4595547
by guest on 13 Nove...

Key questions
What is already known?
Critical illness is common throughout the world and COVID-19 has caused a global surge of critically ill patients.
There are large gaps in the quality of care for critically ill patients, especially in low-staffed and low-resourced settings, and mortal...

In 2015, the United Nations set important targets to reduce premature
cardiovascular disease (CVD) deaths by 33% by 2030. Africa disproportionately
bears the brunt of CVD burden and has one of the highest risks of dying
from non-communicable diseases (NCDs) worldwide. There is currently
an epide...
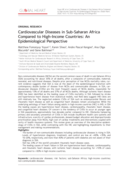
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...

Guidelines for the care and treatment of persons diagnosed with chronic hepatitis C virus infection


published in: Viruses 2016, 8, 161

Model Chapter for textbooks for medical students and allied health professionals

Canadian Journal of Microbiology 25 June 2021 https://doi.org/10.1139/cjm-2020-0572
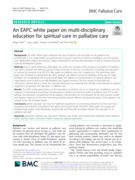
The EAPC White Paper addresses the issue of spiritual care education for all palliative care
professionals. It is to guide health care professionals involved in teaching or training of palliative care and spiritual care; stakeholders, leaders and decision makers responsible for training and educati...
We will soon be piloting a project titled “Integrating Spirituality into Patient Care” that will form “spiritual care teams” to assess and address patients’ spiritual needs in physician outpatient practices within Adventist Health System, the largest Protestant healthcare system ...