Filter
7420
Filtered Results: 7420
Text search:
policy-making
Featured
Recommendations
567
New Publications
1972
Language
Document type
No document type
4104
Studies & Reports
1417
Guidelines
841
Manuals
429
Strategic & Response Plan
313
Training Material
122
Fact sheets
113
Situation Updates
40
Resource Platforms
13
Infographics
10
Brochures
9
Online Courses
4
Videos
3
App
2
Countries / Regions
Global
367
India
268
Kenya
243
Ethiopia
171
South Africa
157
Nepal
156
Uganda
155
Myanmar / Burma
152
Nigeria
147
Sierra Leone
141
Western and Central Europe
139
Liberia
128
Zambia
115
Bangladesh
110
Malawi
109
Rwanda
102
Africa
102
Ghana
101
Tanzania
99
Latin America and the Carribbean
93
Syria
83
Namibia
82
Ukraine
74
Philippines
59
Congo, Democratic Republic of
57
Lesotho
55
Indonesia
51
Asia
50
Zimbabwe
49
South–East Asia Region
47
Cambodia
46
South Sudan
45
Eastern Europe
44
Mozambique
41
Guinea
36
Botswana
36
Haiti
33
East and Southern Africa
31
West and Central Africa
30
Senegal
29
Afghanistan
27
Pakistan
26
Cameroon
25
Germany
25
Middle East and North Africa
25
Russia
25
Yemen
25
Burkina Faso
24
Eastern Europe and Central Asia
24
Brazil
24
Eswatini/ Swaziland
24
Venezuela
23
Sudan
20
Lebanon
19
Central African Republic
19
Thailand
17
Jordan
17
Western Pacific Region
15
Colombia
14
Benin
14
Vietnam
12
Moldova
12
Somalia
12
China
11
Peru
11
Turkey
10
Laos
10
USA
10
Iraq
10
Albania
9
Côte d’Ivoire / Ivory Coast
9
Mali
9
Sri Lanka
8
Palestine
8
Tajikistan
7
Chile
7
Iran
7
North America
7
United Kingdom
7
Southern Africa
7
Libya
7
Mexico
6
Niger
6
Burundi
6
Hungary
6
Paraguay
6
Papua New Guinea
6
Georgia
6
Poland
6
North Macedonia
5
Timor Leste/ East Timor
5
Jamaica
5
Argentina
5
Egypt
5
Romania
5
Gambia
4
Italy
4
Armenia
4
Tunisia
4
Portugal
4
Greece
4
Bhutan
4
Ecuador
4
Madagascar
4
El Salvador
3
Togo
3
Canada
3
Fiji
3
Kyrgyzstan
3
Morocco
3
Croatia
3
Turkmenistan
3
Spain
3
Honduras
3
Chad
3
Guatemala
3
Serbia
2
Singapore
2
Estonia
2
Malaysia
2
Qatar
2
Bulgaria
2
Lithuania
2
Saudi Arabia
2
Japan
2
Mauritius
2
Bolivia
2
Nicaragua
2
Slovakia
2
Angola
2
Switzerland
1
Kazakhstan
1
Mongolia
1
Dominican Republic
1
Guinea-Bissau
1
Ireland
1
Gabon
1
Denmark
1
France
1
Maldives
1
Norway
1
Morocco
1
Azerbaijan
1
Belarus
1
Israel
1
Bosnia and Herzegovina
1
Belize
1
Costa Rica
1
Panama
1
Djibouti
1
Authors & Publishers
Publication Years
Category
Countries
2815
Key Resources
518
Public Health
422
Women & Child Health
418
Clinical Guidelines
405
Capacity Building
137
Pharmacy & Technologies
54
Annual Report MEDBOX
2
Toolboxes
HIV
560
Mental Health
546
COVID-19
538
Planetary Health
364
Disability
357
TB
312
Conflict
228
Caregiver
208
AMR
181
Refugee
168
Global Health Education
162
NTDs
140
Ebola & Marburg
138
Health Financing Toolbox
124
Pharmacy
122
NCDs
112
Rapid Response
111
Natural Hazards
93
Malaria
91
2.0 Rapid Response
82
Social Ethics
54
Specific Hazards
44
Polio
39
Zika
27
Cholera
23
Typhoon
4
South Sudan
1
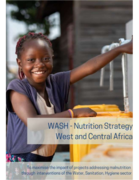
This document was prepared by UNICEF Regional Office for West and Central Africa, under the leadership of Christophe Valingot and the review of Joachim Peeters (WASH Specialist) and Arnaud Laillou (Nutrition Specialist), on behalf of the WASH Regional Group and the Nutrition Regional Group.
This ...

Ethiopia has been repeatedly affected by conflict, flooding, drought, and disease outbreaks in the past years. As of January 2024, the country is actively responding to the longest recorded cholera outbreak which started in August 2022, recurrent measles outbreaks which started in August 2021, and t...

In 2015, the United Nations set important targets to reduce premature
cardiovascular disease (CVD) deaths by 33% by 2030. Africa disproportionately
bears the brunt of CVD burden and has one of the highest risks of dying
from non-communicable diseases (NCDs) worldwide. There is currently
an epide...

The majority of Countdown countries did not reach the fourth Millennium Development Goal (MDG 4) on reducing child mortality, despite the fact that donor funding to the health sector has drastically increased. When tracking aid invested in child survival, previous studies have exclusively focused on...

Food environments are usually defined as the settings with all the different types of
food made available and accessible to people as they go about their daily lives.
That is, the range of food in supermarkets, small retail outlets, wet markets, street
food stalls, coffee shops, tea houses, s...
Non-communicable diseases (NCDs) are the second common cause of death in sub-Saharan Africa (SSA) accounting for about 35% of all deaths, after a composite of communicable, maternal, neonatal, and nutritional diseases. Despite prior perception of low NCDs mortality rates, current evidence suggests t...

The document "Combating False Information on Vaccines: A Guide for Health Workers" is designed to help health workers address vaccine misinformation. It begins by defining misinformation and explaining why it spreads rapidly, often due to its emotional appeal and simplistic explanations. The guide i...

Malaria remains a significant public health concern in the SADC region, accounting for 20% of childhood deaths, as well as prompting numerous outpatient visits and hospitalisations. Around three-quarters of the population, including 35 million children under the age of five and 8.5 million pregnant ...


UNICEF Strategic Plan 2018-2021. Draft Theory of Change Paper



Background paper for the Oslo Summit on Education for Development.
This paper covers the four topics of the Oslo Summit: investment in education, quality of learning, education in emergencies and girls’ education. Disability continues to be one of the primary causes of educational disadvantage a...


Saving Lives Through Safe Surgery (SaLTS)

Transforming the Quality of Health Care in Ethiopia

The ICOPE Implementation Framework provides a score card to help assess the overall capacity of health and social care services and systems to deliver integrated care in community settings and support the development of ICOPE implementation action plans. There are 19 actions needed to implement ICOP...